PRIORITISATION OF TECHONOLOGIES
RESULTS
PARTICIPATION
Of a total of 37 panellists contacted, 33 (89.2%) agreed to participate. Of these 33, 29 (87.8%) finally returned the completed questionnaire. Among those participating, there were 12 managers/administrators (41.4%), 11 clinicians (37.9%) and 6 end-users (20.7%). In all, there were 18 men (62.1%) and 11 women (37.9%).
PRIORITISATION CRITERIA AND WEGHTHING OF DOMAINS
Of the 14 criteria proposed for inclusion in the tool, 3 proved doubtful, with a median score of 6 points. After consulting the working group, it was decided that these 3 criteria should be excluded from the tool. The remaining questions received median scores of 7 to 8 points (one received a score of 9). Insofar as weighting was concerned, the population/end-users domain received a weight of 30%, that of technology 20%, that of risk/benefit 30%, and that of costs, organisation and other implications 20%.
RESULTS BY REFERENCE TO PANELLIST PROFILE
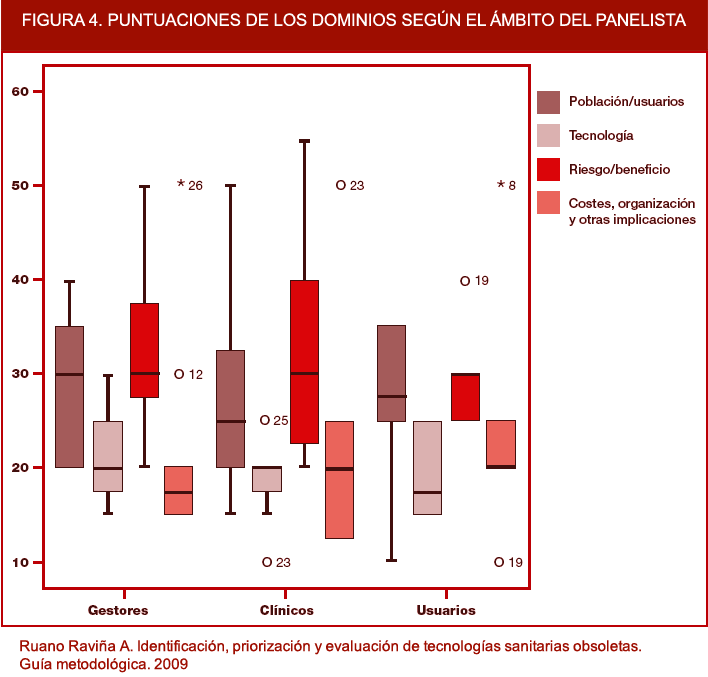
The following figure shows the weightings for each domain according to panellist profile. There were no significant differences in the weightings allocated to the different domains according to panellist profile, and perhaps the most noticeable fact was that clinicians scored the population/end-users domain the lowest, while managers were the ones who awarded the lowest scores to the aspects of costs, organisation and other implications. In terms of gender, there were no important differences in the weighting of the domains, with the maximum differences being 5 percentage points. Shown in Figure 4 are the domain scores awarded by panellists according to their group affiliation.

Figura 4. Domain scores according to panellist profile.
FINAL DOMAINS AND WEIGHTHINGS
After having analysed all the responses of the panellists, the resulting 11 criteria and 4 domains were reduced to 10 criteria and 3 domains. Elimination of an extra criterion (technological alternatives, defined as "authorised technological alternatives existing for the same indications as the potentially obsolete technology") was due to the fact that there was overlapping between this criterion and the definition of obsolete technology itself, so that it was eliminated. On this criterion being eliminated and the other two being regarded by the panellists as doubtful, the domain was eliminated. Elimination of this domain proportionally increased the weighting in the remaining domains and, moreover, maintained the differences among them. Thus, the population/end-user domain had a weighting of 36.66%, that of risk/benefit 36.66%, and that of costs/organisation and other implications 26.67%. The domains and definitive prioritisation criteria, together with the weightings received for each domain, are shown below.
| Table 2. Prioritisation tool domains and criteria. | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Population/end-user domain of prioritisation tool. | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Disease frequency | The condition or indication for which the potentially obsolete technology can be used is frequent (high prevalence and/or incidence). | |||||||||
| Disease burden | The condition or indication for which the potentially obsolete technology can be used amounts to a considerable health loss for the patient (mortality, morbidity, disability). | |||||||||
| Frequency of use of technology | The potentially obsolete technology is currently applied to a high number of patients. | |||||||||
| Patient preferences | There is scientific evidence of a lower acceptance by patients of the potentially obsolete technology versus other existing technological alternatives (e.g., greater unpleasantness, greater discomfort, longer treatments). | |||||||||
| Risk/benefit domain of prioritisation tool. | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Efficacy/Effectiveness/Validity | The scientific literature indicates that the potentially obsolete technology displays less efficacy or effectiveness than other alternative technologies. If it is a diagnostic technology, the potentially obsolete diagnostic test is less valid (yields more false positives and negatives than other available diagnostic tests). | |||||||||
| Adverse effects | There is evidence in the literature of more adverse or more important effects with the potentially obsolete technology versus other existing technological alternatives. | |||||||||
| Risks | The potentially obsolete technology poses a higher likelihood of health-care staff falling ill or having a work accident (e.g., radiations) or of a greater environmental hazard (e.g., waste) than do other existing technological alternatives. | |||||||||
| Costs domain, organisation and other implications of the prioritisation tool. | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Efficiency | There are financial evaluation studies that are more favourable for other existing technological alternatives. | |||||||||
| Maintenance costs | The potentially obsolete technology requires more resources for its functioning (e.g., consumables, reviews, human resources, etc.) versus other existing technological alternatives. | |||||||||
| Other implications | It is foreseeable that withdrawal of the potentially obsolete technology will have a positive impact on the ethical, cultural and/or legal sphere. | |||||||||
| Table 3. Weighting of scale domains | |
|---|---|
| DIMENSION | WEIGHTING |
| Population/end-users | 36,66 |
| Risk/benefit | 36,66 |
| Costs, organisation and other implications | 26,67 |
| Total (1+2+3) | 100% |