PRIORITISATION OF TECHONOLOGIES
METHODS
A brief description is given below of the methodology used to create the obsolete health technology prioritisation tool.
CHHOICE OF METHODS
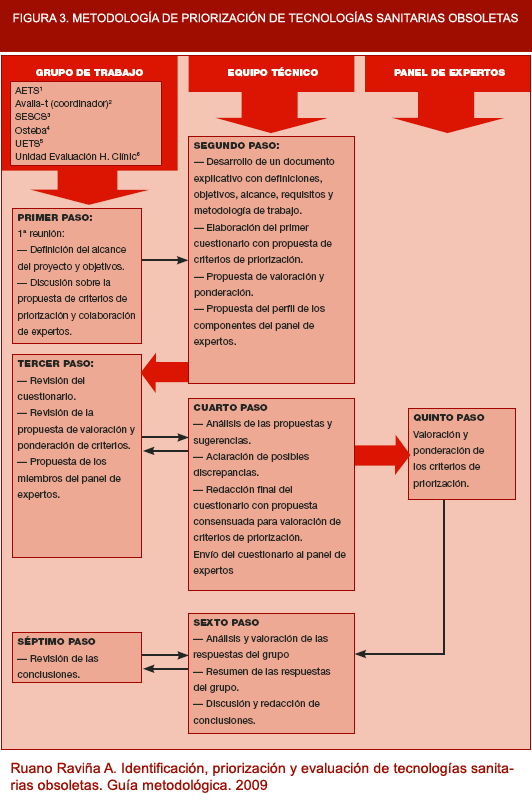
To prioritise obsolete health technologies, 3 work levels were defined, each with its specific tasks (see Figure 3). These work levels were:
- Technical team: made up of technical staff from avalia-t, tasked with . drawing up the prioritisation subproject.
- Working group: made up of experts from the participant assessment . agencies and units. This group analysed the prioritisation criteria and conducted a preliminary evaluation of their inclusion or exclusion. The working group and technical team proposed the component members of the panel of experts.
- Panel of experts: made up of persons exclusively chosen to participate . in the process of prioritisation of potentially obsolete technologies. The members of the panel of experts selected, scored and weighted the final prioritisation criteria.

Figure 3. Methodology for prioritisation of obsolete health technologies.
CHOICE OF PRIORITISATION INSTRUMENT ITEMS AND DOMAINS
The technical team selected a series of items to be used as prioritisation criteria. Dating from the dispatch of the preliminary prioritisation criteria, the members of the working group then had 15 days to make their assessments and comments. Eighteen prioritisation criteria divided into 4 domains were initially selected, and these were then sent to the members of the working group for their assessment. The working group decided that four of these items were to be eliminated. Finally, 14 criteria were included in the prioritisation questionnaire sent to the panellists. Two versions of the prioritisation criteria were drawn up: one for panellists in the clinical and management area, with more experience in health terms; and another, with terminology adapted to health-care system end-users, to make it easier to understand the technical jargon used.
The prioritisation criteria sent to panellists were classified into 4 domains, namely: a) population/end-users (4 elements); b) technology (3 elements); c) risk/benefit (3 elements); and, d) costs, organisation and other implications (4 elements).
SELECTION OF CRITERIA, AND SELECTION AND PROFILES OF PANELLISTS
Panellists were selected by the members of the working group among health-care system clinicians, managers and end-users, and an attempt was made to ensure that the composition of the panel struck a balance with respect to these three groups. The panellists were thus persons drawn from Spain's respective autonomous regions. Among the clinicians, an effort was made to ensure that there was representation of practitioners involved in both primary and specialised care and that, within the specialist group, there were highly technological specialisations. Among the managers, value was attached to the presence of hospital administrators and administrators of central services of the Regional Health Authorities (and among the latter, those most closely linked to the service portfolio, i.e., health care, health assurance, public health, etc.). Finally, among the system end-users it was sought the presence of patient associations, consumer and end-user organisations, expert advisory groups and community participation groups.
Each agency or working group unit chose 6 to 9 potential panellists to participate in the prioritisation process. The task assigned to the panellists was that of selecting the final criteria from among the 14 proposed prioritisation criteria. These criteria were scored from one to nine in accordance with their importance in the panellist's view. In addition, panellists were asked to allocate a weight to each of the four domains in percentage terms, so as to be able to weight the importance of each of the prioritised technologies. A total of 37 panellists were contacted, made up of 13 clinicians, 14 managers and 10 end-users.
ITEM AND DOMAIN SCORES AND WEIGHTHINGS. ANALYSIS OF RESULTS
The avalia-t secretariat contacted the panellists individually by telephone or e-mail, in order to invite them to take part in the project and explain its purpose. To maximise participation, the number of contact attempts per panellist was variable. All prioritisation questionnaires were sent and received by e-mail.
Once the scores and weightings had been received by avalia-t, the responses were analysed and each domain weighting was calculated. The results were forwarded to the working group for comment and discussion.
Scores were classified into: a) 7-9 points, clearly important criterion; b) 4-6 points, criterion with doubts regarding its importance; and, c) 1-3 points, criterion of little importance. Where any element received a median score of 3 or lower, it was excluded from the prioritisation criteria.
DEVELOPMENT OF PRIORITISATION TOOL
After the prioritisation scale had been agreed upon and finalised, it was decided that a software application, known as the PriTec tool, be created, so that scores received by several potentially obsolete technologies could be compared and the technologies then prioritised. This application, funded by the Galician Health Authority's Directorate-General for Health Assurance & Planning (Dirección Xeral de Aseguramento y Planificación Sanitaria de la Consellería de Sanidade, Galicia), complements the work done by the technical team and working group. The application displays the results both quantitatively and graphically. It enables technologies to be assessed on the basis of pre-established criteria and the results obtained after weighting the domains to be calculated. In addition, it also allows for comparison of the scores received, both overall or broken down by domain, for each technology assessed. This tool can be accessed at the websites http://www.pritectools.es or http://www.pritectools.com, and is available for public use, free of charge, to all those wishing to use it.